Knee pain: ‘The hidden lesions’ and novel treatments
Knee pain and osteoarthritis (knee OA) impact hugely on quality of life. Drawing from clinical experience and research studies, Professor Shaw-Ruey Lyu and colleagues at the School of Medicine, Tzu-Chi University, Taiwan, describe ‘the hidden lesions’ of knee OA and propose the concept of Knee Health Promotion Option (KHPO) for effective treatment. The team highlight the role of medial abrasion phenomenon (MAP) in the pathogenesis of knee OA, and advocate use of two techniques to eliminate MAP, reduce knee pain, improve quality of life, and even halt the deterioration process of knee OA for patients.
The largest joint in our bodies, our knees, are under immense strain; they carry the weight of our bodies and continuously undergo bending and extension. In the elderly, knee osteoarthritis (knee OA) is one of the main causes of mobility issues with an estimated prevalence of 10% in men and 13% in women over the age of sixty, affecting over 250 million people worldwide. Prevalence of knee OA has increased recently, due in part to higher obesity rates and a sedentary lifestyle. Other predisposing factors for the condition include a history of knee injury, age, and joint instabilities that increase mechanical stress. Mechanical stresses play a key role in the degradation of cartilage with some stresses affecting cartilage matrix synthesis. Extremely high stress can elicit an ‘injury response’ leading to cell death and increased degradation. In addition to impacting patients’ quality of life, this progressive disease imposes a significant financial burden.
Thought to be multifactorial in origin, the causes and pathogenesis of knee OA are not fully understood. Pain is a major symptom of knee OA with chronic pain often leading to reduced activity which, in turn, causes weight gain and more pain. Therapeutic interventions exist and successes are higher when disease is treated in the early stages. Patients with end-stage disease may undergo total knee replacement. Knee OA is now recognised as a whole joint disease as it is not just the articular cartilage that is affected (although this is a major pathological feature) but also the supporting subchondral bone and tissues in the joint. Synovitis (swelling of the synovium, the lining of the joint), also a key feature of knee OA, is associated with knee pain severity. The medial plica is a fold in the synovium which, if inflamed, thickened, and fibrous, can cause pain. Early studies by Professor Shaw-Ruey Lyu, Tzu-Chi University, Taiwan, implicate medial plica in the pathogenesis of knee OA and severity of disease is associated with the severity of medial plica fibrosis and the patient’s age.
Drawing from their clinical observations and through their research studies, Lyu and colleagues have further described the important but neglected issue of the medial abrasion phenomenon (MAP). MAP arises during knee motion, where the medial plica has repetitive contact and friction with the medial femoral condyle opposite it. MAP is one element of what Lyu describes as ‘the hidden lesions’, so called because synovitis makes it difficult to see during knee arthroscopy. Through a series of studies, Lyu’s research team describe and demonstrate the role of MAP in the pathogenesis of knee OA. They also describe two techniques: arthroscopic medial release (AMR) and arthroscopic cartilage regeneration facilitating procedure (ACRFP), to treat knee OA. Lyu argues that if implemented early enough, these techniques enable the removal of the unfavourable environment where an imbalance in cartilage metabolism occurs, leaving an environment that allows the cartilage to regenerate and repair itself.
Lyu presents evidence that the hidden lesions, especially MAP, contribute to knee OA pathogenesis.
‘The hidden lesions’
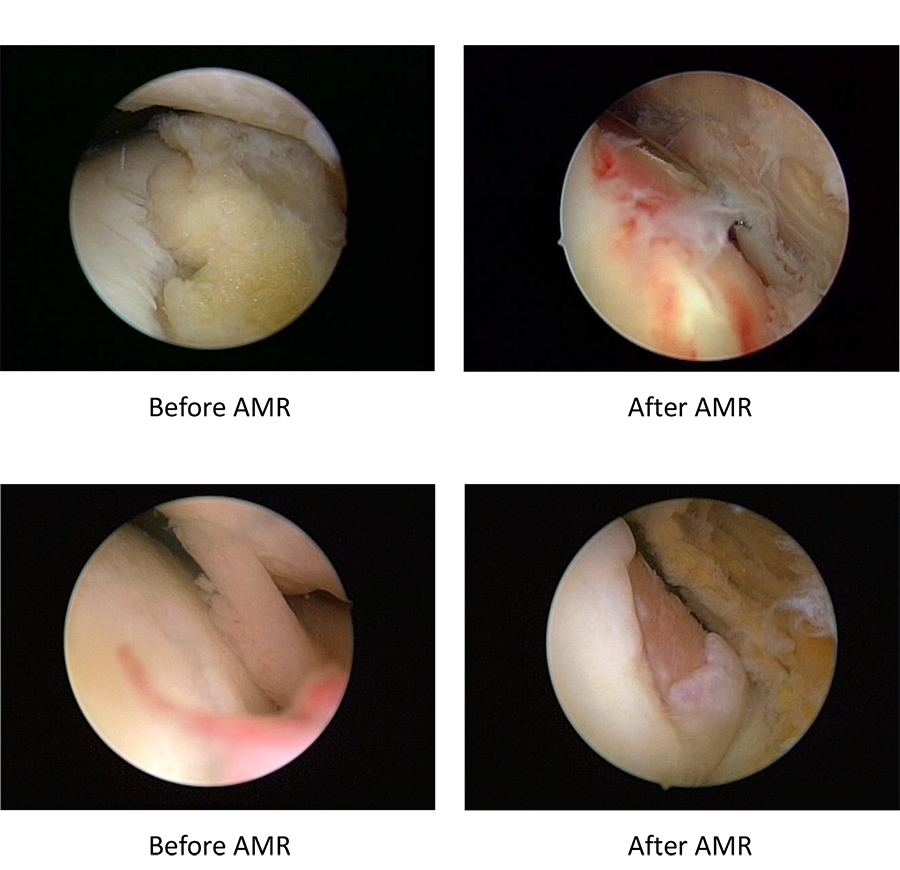
The hidden lesions are cartilaginous lesions only visible after the removal of the synovial tissue and the medial plica (figure 1). Studies propose that these lesions play a role in knee OA and Lyu suggests that his team’s discovery has led to improvements in the treatment of knee OA. Medial plica-related medial abrasion syndrome (MAS) is the clinical manifestation and symptoms of MAP which is caused in turn by the medial plica lesion. Lyu has aimed to better understand the biomechanical effects caused by MAP, histological characteristics, and biochemical analysis of the affected medial plica.
Lyu’s models indicate that fibrotic medial plica causes abrasion or shedding when in close contact the medial femoral condyle and this abrasion in turn also causes injury to the medial plica itself. This abrasion triggers proinflammatory cytokine release in medial plica, specifically interleukin 1- (IL 1-) leading to increase matrix metalloproteinase -3 (MMP-3). MMPs are enzymes that can degrade cartilage matrix. Subsequently, normal cartilage metabolism ceases and the balance shifts towards catabolic processes or degradation. Lyu’s team also showed that the concentrations of TNF- (a pro-inflammatory cytokine), MMP-3, and IL-1 in synovial fluid are higher in the medial compartment than in the lateral compartment of the osteoarthritic knees, indicating that medial abrasion is present in knee OA.

These results provide further evidence implicating MAP in knee OA pathogenesis (figure 2).
Use of novel techniques
Lyu and colleagues propose the use of AMR as a treatment of knee OA in the medial compartment. This procedure aims to stop the friction between the medial plica and medial femoral condyle and to relieve the stress between the cartilage which is the after-effect of chronic inflammation. This could alleviate the pain suffered by patients and even halt the deterioration process of knee OA. The team also advocate the use of a novel technique, ACRFP – a combination of AMR and traditional procedures – to treat the whole osteoarthritic knee.
In a study published in the journal Medicine, Lyu’s research team report the prevalence and clinical characteristics of MAS in middle-aged to older individuals, who more commonly suffer from chronic knee pain, significantly degrading their quality of life. In younger individuals, medial plica syndrome is a common cause of knee pain while OA is the most common cause in middle- to old age. There has been little research on MAS in middle to older-aged patients. Lyu’s study revealed for the first time the high prevalence (95%) of medial plica in middle to old age individuals with chronic knee pain, most of whom had concomitant OA. Patients treated with AMR and followed for three years reported a satisfaction rate of 85%. The study, also the first to report the radiological findings of MAS and its concomitance with OA in this population, demonstrated the positive effects of AMR in alleviating knee pain related to MAS and knee OA.


Figure 3. Radiographic evidence of cartilage regeneration after arthroscopic cartilage regeneration facilitating procedure (ACRFP).
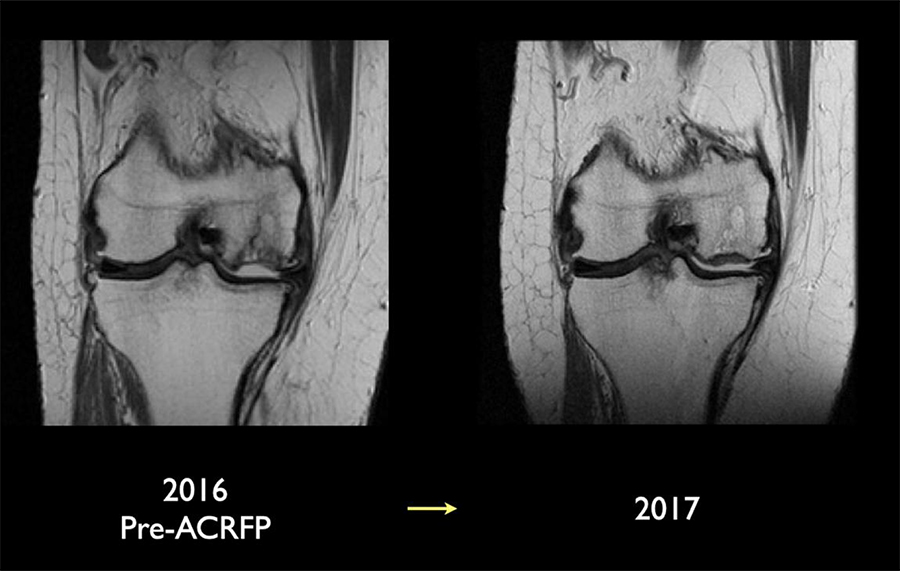
In another study, Lyu and his colleagues followed patients with knee OA for three years post-ACRFP, measured and recorded their knee society score (KSS) and knee injury and osteoarthritis outcome score (KOOS). The team then made a pre- and post-treatment comparison of these scores. The outcome showed that 91% of patients, even in those with advanced (stage IV) disease, were satisfied with the treatment. Post-treatment Improvements in KSS and KOOS scores were identified, indicating relief of symptoms and improvement of quality of life. The radiographic outcome analyses indicated reversal of cartilage degeneration in 80% of patients (figure 3) while the MRI outcome study indicated reversal of cartilage degeneration in 72% of patients (figure 4).
The researchers suggest that ACRFP stops both the physical damage caused by MAP and the resultant detrimental biochemical effects of MAP, and if maintained properly in post-operative care, the cartilage has a favourable environment for its regeneration. ACRFP intervention at an early stage and proper post-operative management are important for the procedure to be successful. Lyu and his colleagues argue that their proposed interventions (AMR and ACRFP) possess substantial rationale for clinical use and, given their promising results so far, offer hope for knee OA patients. Now, clinical trials and longitudinal MRI studies are required to confirm these findings and further knowledge in this field.
Their discovery and proposed interventions (AMR and ACRFP) possess substantial rationale for clinical use.
MAP and persistent post-operative pain
Persistent post-operative pain (PPOP) occurs in up to one third of patients who have undergone partial, or unicompartmental knee arthroplasty (UKA), or total knee arthroplasty (TKA). Radiography may indicate the reason for PPOP but sometimes patients report pain or discomfort even in the absence of any obvious radiographic indications. The surgery may radiographically appear successful, yet the patient is still unsatisfied. Lyu hypothesises MAP to be a cause of PPOP which could be prevented by eliminating MAP during UKA or TKA. He also suggests that PPOP could be alleviated by eliminating MAP using AMR post UKA or TKA if required. Lyu’s researchers performed UKA and TKA where MAP was also eliminated at the time of surgery and reported a very low incidence of PPOP in these patients. In addition, they described a separate group of patients whose MAP had not been removed at the time of their UKA or TKA, performed by surgeons unrelated to Lyu’s team, and who later come to him with a complaint of PPOP. For these patients, Lyu eliminated their MAP in a AMR after their primary surgery. These patients reported high satisfaction levels after such AMR procedure. These findings highlight the importance of MAP in patients with PPOP after arthroplasty.
Overall, Lyu presents evidence that the hidden lesions, especially the MAP, contribute to the pathogenesis of knee OA. Identification of MAP and early intervention using AMR and ACRFP can prevent further degradation and improve quality of life. He argues that even in later stages of the disease, ACRFP could prevent the need for the implantation of prosthesis and enable the patient to keep their natural knees. Based on the experience gained from clinical encounters and through research, the team at Lyu’s centre have put forward the notion of the KHPO, a suggested protocol for the comprehensive treatment for knee OA. As is often said, ‘prevention is better than cure’, so Lyu and colleagues propose to promote behavioural modifications in the general public to help reduce MAP and the subsequent incidence of knee OA.
Personal Response
How do you plan to take forward these findings into the next stage of research and will this be in the form of clinical trials and imaging studies?
It’s more likely to be in the form of imaging studies. We had not pursued a standard randomised clinical trial, mainly for humanitarian reasons. Over the span of more than 20 years, my novel treatment has relieved more than 10,000 patients of their knee pain. I know that this treatment works, so I cannot bring myself to attempt a full clinical trial because I cannot conscientiously assign any subject to the control group, which deprives the subject of the opportunity to receive my treatment in a timely manner and leaves them to suffer and face a likely TKA in future.