Using patient datasets to track COVID-19 prevalence
Obtaining an accurate picture of COVID-19 cases has provided a major challenge throughout the pandemic. Changes in testing methods and skewed selection of higher-risk groups may bias the results. Dr Amy Hou, Dr Genevieve Pang, and Dr Lorrin Pang at the Hawaii State Department of Health, Maui District Health Office, US, propose a novel way to estimate local prevalence of COVID-19. Patients who attend healthcare settings for routine procedures are tested for COVID-19 regardless of their level of risk. This broad set of individuals may offer a robust marker group for COVID-19 trends, reducing bias in reporting and providing reliable data to inform and monitor public-health interventions.
Since the start of the global COVID-19 pandemic, there have been almost 550 million confirmed cases of the disease, caused by the SARS-CoV-2 virus. The rapid spread, alongside the constant evolution of viral strains, has presented significant challenges to tracking the true prevalence of this disease.
In addition, the way we test for COVID-19 is adapting and changing as more is learnt about the virus and new technologies become available. Different countries and governments use different testing and reporting systems, making it almost impossible to compare COVID-19 infection levels.
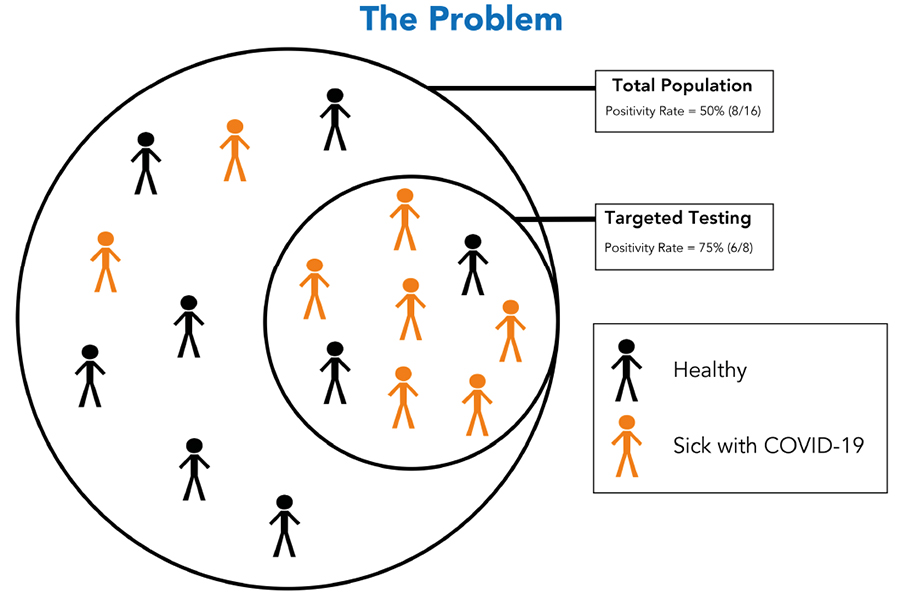
Some of the testing methods can also result in bias. For example, at the beginning of the pandemic, limited numbers of testing kits were provided to high-risk individuals, such as healthcare workers and individuals who had been exposed to known cases of the virus. This in itself produced more positive results and was unlikely to be an accurate representation of COVID-19 cases in the wider population.
Different countries and governments use different testing and reporting systems, making it almost impossible to compare COVID-19 infection levels.
Researchers at the Hawaii State Department of Health explain that as diagnostic testing became more widely available, COVID-19 cases appeared to decrease. However, it is unclear whether this was an accurate observation or whether the inclusion of lower-risk individuals can lower the overall average number of positive cases. Dr Amy Hou, Dr Genevieve Pang, and Dr Lorrin Pang also point out that home testing kits are often excluded from reported cases.
Overall, the biases within estimates of COVID-19 prevalence derived from these frequently changing, high-risk populations may result in inaccurate conclusions and poor-fitting public-health policies for the management of COVID-19.
Reducing bias
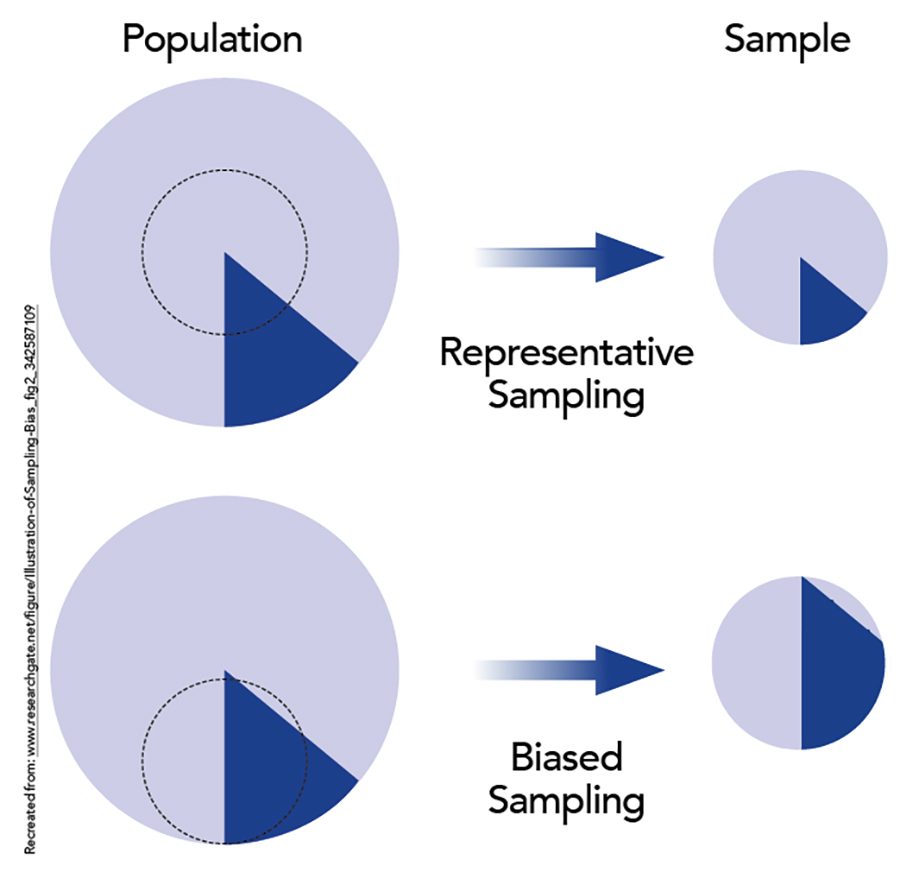
Previous studies have already explored the idea that a large number of randomly selected individuals must be followed to accurately determine the baseline prevalence of COVID-19 within a community. In practice, this is often difficult to achieve, as certain population demographics may be more likely to engage with the study and bias the results.
The research team proposes a novel approach to overcoming many of the factors that can bias reported COVID-19 prevalence rates. They have identified a group of individuals which is required to undergo routine COVID-19 screening before elective procedures or operations, termed the pre-procedural or pre-operative group. These types of patients are afflicted with conditions independent of COVID-19 and are neither positively nor negatively biased. This group does not have the option to opt in or out of testing and spans a wide demographic of high- and low-risk individuals.
The researchers conclude that this pre-procedural group is likely to better represent a randomised approach to testing that is unlikely to dramatically change over time. They suggest that this group may offer a robust surrogate marker for randomisation to track infection rates within a community. In addition, many medical facilities already hold this information on a large number of patients, allowing retrospective analysis of COVID-19 rates over time.

based on indications that are neither positively nor negatively biased with respect to COVID-19 risk.
Pre-procedural testing
Hou and colleagues accessed existing patient data collected by the Maui Medical Group (MMG) clinics on the island of Maui, which is part of Hawaii, USA. The MMG has a patient base of around 35,000–40,000 patients, representing 20–25% of the island’s population.
The data included 12,640 COVID-19 test results collected between May 2020 and March 2021. The researchers also obtained information about the age and gender of the patients, as well as the reason for testing. Those who fell into the pre-procedural group were individuals who required a COVID-19 test before undergoing routine procedures, including hip or knee replacements, endoscopies, or general surgery, such as gallbladder removal.
Using these data, the results were broken down into smaller subsets to better understand how specific groups contributed to overall reported COVID-19 cases. For example, were higher reported rates of COVID-19 mainly due to higher numbers in symptomatic patients, or those who had recently travelled abroad?
The results showed that most patients underwent COVID-19 testing because it was a requirement ahead of a medical procedure. Others had symptoms of COVID-19 or had been exposed to someone with the disease.

During this time period, the researchers concluded that around 0.1% of pre-procedural groups tested positive for COVID-19. This contrasted with 3.9% of individuals with symptoms and 4.2% of individuals exposed to a known COVID-19 positive case. Overall, around 2% of the total study population had a positive test result.
The pre-procedural group contained fewer positive test results, although the number of positive test results did increase over time, regardless of which group was examined. The researchers explain that pre-procedural groups may show different patterns compared to a subset of selected high-risk patients (those with COVID-19 symptoms or known exposure) with positive COVID-19 bias. Taking this into account, pre-procedural groups offer a sample population with less bias, but which still show the same trends over time, allowing reliable tracking of COVID-19 prevalence.
This pre-procedural group may offer a robust surrogate marker to track infection rates within a community.
While this pre-procedural group spanned a broad range of individuals who were not acutely ill, it could be speculated that any individual who is receiving input from a healthcare setting may be more likely to be older, from a lower socioeconomic background or have other physical, mental, or social complications. Indeed, Hou and colleagues identified that these patients may be more cautious when meeting with others or leaving their homes, in view of their upcoming medical appointments. They suggest that correction factors and adjustments may be required when modelling the reported data to account for this.
A robust marker group for COVID-19 trends
A truly randomised sample is the gold standard to eliminate bias for estimating COVID-19 rates in communities. However, this type of sample is unfeasible because it typically requires months to collect, while COVID-19 rates are changing daily. Hou and colleagues offer an attractive way to monitor infection trends over time. The researchers argue that pre-procedural groups can serve as a robust marker to the randomised group and provide vital insights into a large, more representative subset of the community.
Interestingly, this finding contrasts with other studies that suggest testing should focus on higher-risk groups. The researchers from Hawaii State Department of Health highlight the large discrepancies between estimated prevalence of COVID-19 cases in low- and high-risk populations, meaning that we may not be getting a true picture of infection rates. Targeted testing on high-risk people is an effective strategy to contain COVID-19 outbreaks, but not for describing background rates (also known as latent prevalence). Including a wider selection of individuals, not just those who are more likely to test positive for COVID-19, improves the accuracy of datasets.
Longitudinal data collection is important to track COVID-19 cases over a longer time frame. Accurately tracking true local infection rates is crucial for assessing the efficacy of public-health interventions. Accurate rates are also key to monitor trends in virulence, transmissibility, and severity under conditions of rapidly emerging novel variants of COVID-19.
Learning more about the infection dynamics of COVID-19 helps to predict how the next COVID-19 variant, or other infections, may spread, thus encouraging early intervention and a reduction in illness and mortality. It also highlights an often-underutilised population group that could be harnessed for similar data collections and analysis in the future.

Personal Response
How do you see the use of pre-procedural group testing being used to guide COVID-19 monitoring in other countries or populations?
Other countries can utilise pre-procedural datasets and run analyses of the COVID-19 positivity rates to better understand the true trend of the prevalence and better equip them when making public health policies. If several countries or populations have similar pre-procedural policies, then the data and trends can be compared among those countries or populations – which can help them understand various trends and influx of different variant strains.