Timely insulin therapy to treat type 2 diabetes
This abstract is based on the following article and the references it contains: Hanefeld M., Fleischmann H., Siegmund T., & Seufert J. (2020). Rationale for Timely Insulin Therapy in Type 2 Diabetes Within the Framework of Individualised Treatment: 2020 Update. Diabetes therapy: research, treatment and education of diabetes and related disorders, 11(8), 1645–1666. https://doi.org/10.1007/s13300-020-00855-5
Sugars, i.e. carbohydrates, and more specifically glucose, is the body’s preferred source of energy. When food including carbohydrates is digested and nutrients enter the bloodstream, a hormone called insulin is responsible for moving glucose out of the blood and into cells, where it is broken down to generate energy. Produced by the ꞵ-cells of the pancreas, insulin is essential to control the amount of sugar in the blood. Dysregulations can have severe consequences.

Diabetes is a lifelong condition that causes blood sugar level to be too high (hyperglycaemia). Because there is not enough insulin or because it is dysfunctional, glucose is not moved into cells and broken down into energy. There are two main types of diabetes. In type 1 diabetes, the body’s immune system attacks and destroys the cells that produce insulin. In type 2 diabetes, the body does not produce enough insulin, or the body’s cells are resistant to insulin and therefore do not react to it. While no lifestyle changes can lower the risk of type 1 diabetes, healthy eating, regular exercise and a healthy body weight can delay, prevent or even reverse the development of type 2 diabetes, which is the most common type; in the United Kingdom for example, around 90% of all adults with diabetes have type 2. Professor Hanefeld works on type 2 diabetes.
Professor Hanefeld recommends an individualised therapy taking into account the risk/benefit balance for each patient.
Hyperglycaemia and type 2 diabetes
Mild hyperglycaemia with elevated fasting or postprandial blood glucose at a level below threshold for diabetes is frequently found among people with obesity, hypertension, fatty liver and elevated lipids. The International Diabetes Federation labels that risk category prediabetes. Prediabetes increases the risk of developing type 2 diabetes and even worse the risk of cardiovascular disease and fatty liver. The excessive quantity of sugar requires insulin to be moved out of the blood, more insulin is needed in type 2 diabetes with insulin resistance and when progressing, more insulin than the pancreas can produce. Chronic hyperglycaemia constantly stimulating the production of insulin poses a threat to the ꞵ-cells of the pancreas, has harmful effects on insulin producing cells, and thus, causes deficits in insulin secretion. Then starts a vicious cycle because, with impaired insulin secretion, blood sugar levels spiral out of control, hyperglycaemia worsens and exerts harmful effects on ꞵ-cells, which impairs insulin secretion even more. In addition to deficits in insulin secretion, hyperglycaemia can worsen the development of insulin resistance.
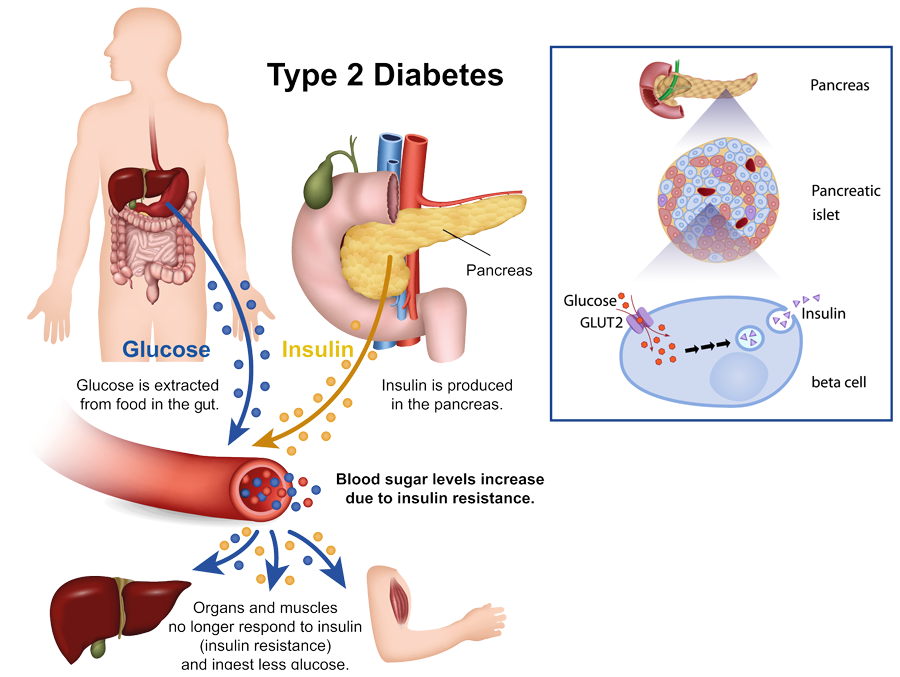
Produced by the ꞵ-cells of the pancreas, insulin is essential to control the amount of sugar in the blood. Alila Medical Media/Shutterstock.com
Diabetes is diagnosed when blood sugar level reaches a certain threshold, but impairment of insulin secretion occurs long before that; the vicious cycle is already on. Besides being responsible for moving glucose out of the blood and into cells, insulin also acts on lipid metabolism: insulin favours the storage of lipids in adipose tissues by inhibiting lipolysis, a process through which fatty acids are released into the bloodstream. Therefore, insulin deficiency leads to excessive blood levels of glucose and fatty acids. Both hyperglycaemia and elevated fatty acids are toxic for ꞵ-cells, to such an extent that in advanced diabetes with a duration of more than 10 to 15 years, residual pancreatic ꞵ-cell function is critically impaired, sometimes like in type 1 diabetes.
Controlling blood sugar levels
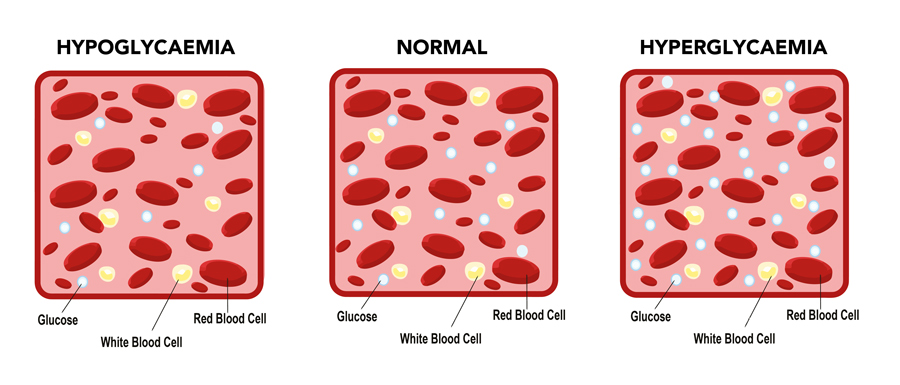
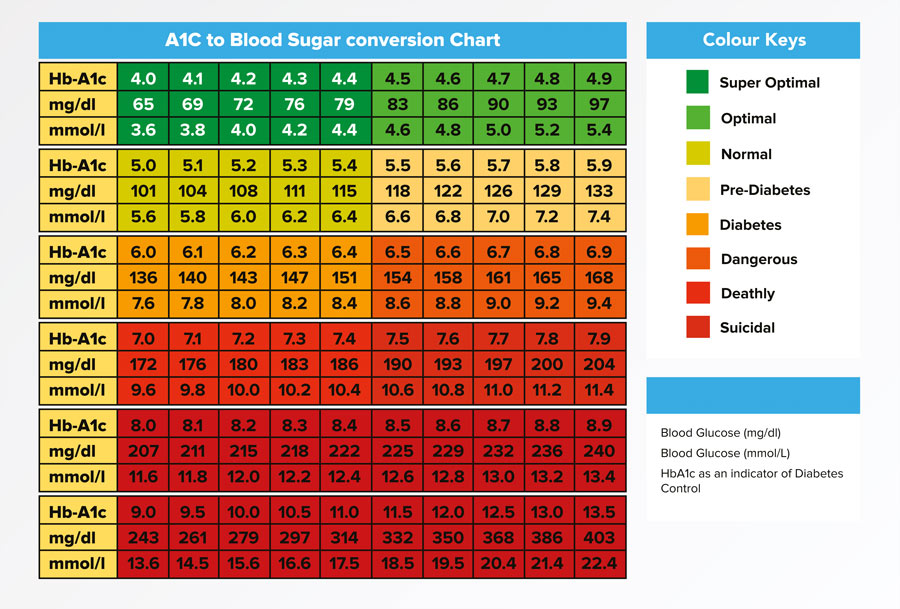
When glucose builds up in the blood, it binds to haemoglobin, the protein found in red blood cells responsible for carrying oxygen throughout the body. This combination of glucose and haemoglobin is called haemoglobin A1c, or HbA1c. The quantity of HbA1c is measured by the HbA1c test that estimates blood glucose levels within the last two to three months. This test is used to diagnose diabetes: while the normal range for the HbA1c level is between 4% and 5.6%, HbA1c levels between 5.7% and 6.4% indicate prediabetes which corresponds to a higher risk of getting diabetes, and levels of 6.5% or higher indicate diabetes. People with diabetes also use this test regularly to monitor their average blood sugar level over the previous two to three months.
Controlling blood glucose level is of utmost importance in the management of type 2 diabetes. While there is no cure for diabetes, treatments aim at maintaining a near to normal blood glucose level. Stability not only avoids hyperglycaemia but also reduces the risk of hypoglycaemic episodes. Indeed, dysregulation of blood sugar levels in people with diabetes can go both ways: in addition to chronic hyperglycaemia, the progression of type 2 diabetes may be associated with higher risk of hypoglycaemia. Both hyperglycaemia and hypoglycaemia are harmful and related to potential cardiovascular and cerebral complications, besides impacting fitness in daily life. Moreover, long-term poor diabetes control has harmful effects on diabetes-related complications such as diabetic kidney disease, retinopathy, diabetic foot and erectile dysfunction.
Oral drugs and insulin
Requiring injections, insulin is usually not the first recommended treatment. Instead, several oral antidiabetic drugs (OAD) have proven their ability to lower blood glucose levels. However, given its physiological nature (i.e. lowering glucose) insulin is stated in guidelines to be the most effective therapy. Moreover, the efficacy of oral drugs decreases over time because as type 2 diabetes progresses, ꞵ-cell failure increases, but a minimum of 15% or 20% of pancreatic ꞵ-cell function is needed for an adequate glucose-lowering effect of most oral drugs. Some guidelines for medical treatment of elderly people with diabetes only recommend the use of insulin if oral drugs fail and HbA1c levels are over 8-10%. However, these recommendations may result in an inadequate delay of insulin treatment.
Benefits of timely insulin therapy
Many patients eventually become insulin-dependent since the diabetes progresses due to progression of insulin deficiency and/or resistance, and OAD treatment may not be sufficient to keep glycaemia under control. Because insulin therapy is often started when other treatment options fail and HbA1c levels are too high, insulin treatment is used late into diabetes progression, so late that individual HbA1c targets are not achieved in the majority of cases. Professor Markolf Hanefeld argues that timely insulin therapy could benefit patients.
Only intensive insulin treatment is able to reliably correct hyperglycaemia within one to two days of treatment. In newly diagnosed diabetes, even in patients with severe hyperglycaemia (HbA1c levels higher than 9%), early insulin therapy is able to achieve near to normal glucose control and leads to long-lasting remissions in up to 50% of patients; some long-term studies showed that insulin is able to keep glucose to a near normal range over an extended period of more than six years.
Timely insulin therapy is also one of the most effective tools to protect ꞵ-cell function: early insulin can delay or reverse ꞵ-cell dysfunction and loss as demonstrated in the ORIGIN study. Short-term intensive insulin therapy also decreases insulin resistance.
Timely initiation of insulin promotes better treatment: when initiated early, lower dosage is necessary, which comes with lower rates of adverse events.
Adverse effects and timing
Hypoglycaemia and weight gain are potential serious adverse effects of inappropriate insulin therapy. Of notice, only minimal weight gain has been observed with second generation basal insulin, e.g. insulin glargine 300 U/mL or insulin degludec. Severe hypoglycaemia may also increase risk of cardiovascular events and arrhythmias. Not at least, insulin therapy requires professional medical care and may be associated with inconveniences for elderly patients.
However, timing is important. Studies showed that severe hypoglycaemic episodes and weight gain are serious adverse events of inappropriate insulin treatment, when insulin therapy is started too late or at high HbA1c levels requiring high dosages, but there is no evidence for a specific risk associated with timely and adequate insulin treatment.
The risk/benefit balance
Safety and quality of life are major issues to be considered at initiation of treatment. Professor Hanefeld recommends an individualised therapy taking into account the risk/benefit balance for each patient.

For patients with very uncontrolled hyperglycaemia (HbA1c > 9%) transitory intensive insulin treatment at diagnosis of diabetes offers a chance of long-lasting remission. Moreover, it could be beneficial because these patients will likely need insulin later when their condition worsens. In advanced diabetes, timely initiation of insulin promotes better treatment: when initiated early enough, lower dosage is possible, which comes with lower rates of adverse events.
Seniors with frailty and sarcopenia are also good candidates for patient-centred timely insulin treatment. Sarcopenia causes a decline in skeletal muscle mass and strength which play a key role in the loss of mobility and the ability of self-care. One of the effects of insulin is improvement of protein synthesis. Therefore, insulin may have anabolic effects that are especially beneficial for elderly with sarcopenia.
Finally, the risk/benefit balance can be improved by limiting the risks. One way to do that is to combine insulin with another antidiabetic drug. Indeed, prevalence and harmful consequences of hypoglycaemic events are attenuated if a drug named metformin is used or continued when initiating basal insulin. Further, second generation long-acting basal insulins offer more safety and convenience under real-world conditions. Timely combination of insulin with other drugs may therefore be considered.
Personal Response
What led you to start working on type 2 diabetes?
We have been very successful at treating diabetes and its complications through lifestyle interventions, new drugs, and controlling glucose in patients. Education, lifestyle intervention and pharmacological control in partnership with informed patients has become my passion as a physician until this day.